Secondary Traumatic Stress, Burnout and Resilience in the Child Welfare Workforce: Early Results from Nebraska’s Randomized Controlled Trial of Resilience Alliance
A 2018 needs assessment indicated that more than 50% of the child welfare workforce in Nebraska was experiencing elevated secondary traumatic stress (STS). STS refers to the experience of people – generally professionals– who are exposed to others’ traumatic events as part of their work. As a result of this exposure, these professionals can develop their own traumatic symptoms and reactions such as sleeplessness and anxiety.
The Nebraska Department of Health and Human Services (DHHS) Division of Children and Family Services (DCFS) in partnership with the Quality Improvement Center for Workforce Development (QIC-WD) implemented CFS Strong, a multi-phased workforce intervention designed to decrease levels of STS symptoms and increase worker retention by improving their resiliency, job satisfaction, and the ability to manage work-related stress. The first phase, implemented in May 2019, included staff’s participation in the 24-week Resilience Alliance (RA) program.
The QIC-WD evaluation team used a cluster randomized controlled trial (cRCT) to evaluate the effectiveness of RA. Supervisory groups (supervisors and workers) were randomly assigned to participate or to not participate in RA, with equal-sized RA (intervention) and not-RA (control) groups. The evaluation team analyzed changes in caseworker and supervisor STS, burnout, and resilience over the 24-week period of RA participation. Participants in both the intervention and the control groups completed the Secondary Traumatic Stress scale, the Maslach Short Burnout Scale, and the Connor Davidson Resilience Scale prior to and at completion of the 24-week period. The QIC-WD evaluation team ran linear, mixed repeated-measures models in SPSS, segmented by years of child welfare work experience.
Caseworker and supervisor attendance at the RA group meetings was good with the median number of sessions attended being 18 of 24 sessions, or 75%. Mixed modeling results show no difference in change over time between the intervention and control groups for STS, burnout, or resilience. However, for some staff subgroups, there may be a protective effect resulting from RA with regard to burnout and resilience.
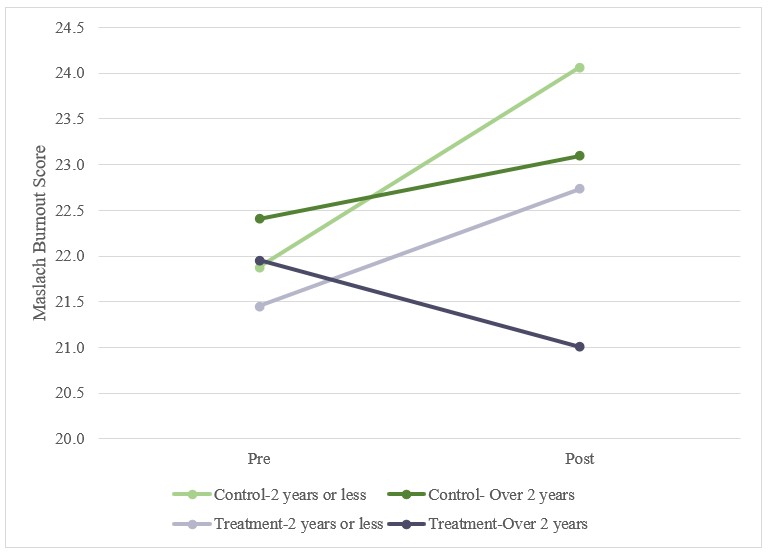
- Among staff with two or fewer years of child welfare experience, those in the intervention group showed flatter burnout rates during RA, while those not participating in RA showed a significant increase in burnout rates (see Figure 1).
Figure 1. Burnout Rate Pre/Post RA
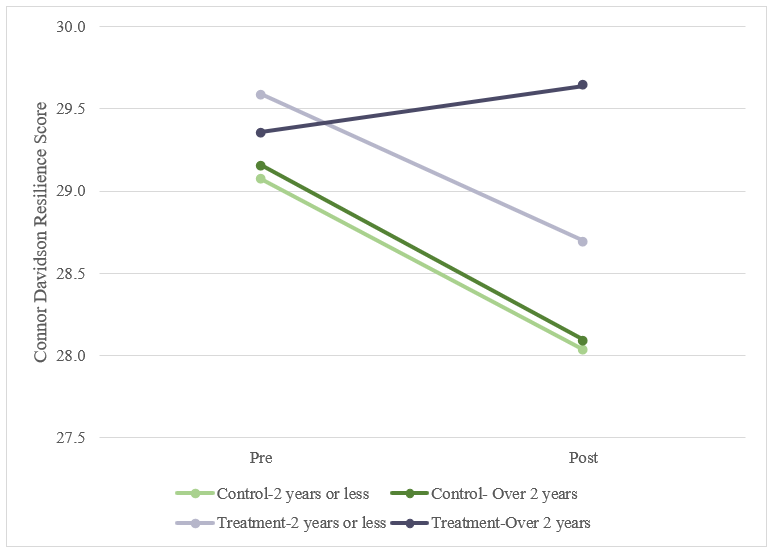
- Among staff with more than two years of experience, those not participating in RA showed a significant drop in resilience, but there was no significant drop among those in the intervention group (see Figure 2).
Figure 2. Resilience Score Pre/Post RA
The QIC-WD believes that this is the first randomized controlled trial of the RA program. It is currently listed on the California Evidence Based Clearinghouse as unable to be rated for evidence of efficacy because it lacks at least one "published, peer-reviewed study utilizing some form of control." Therefore, this study makes a significant contribution to the knowledge base. Although RA may not have been broadly effective across the child welfare workforce in Nebraska, it may indeed offer promise in mitigating burnout and supporting resilience in among some segments of the child welfare workforce.